
Mouth Ulcer: A Specialist Surgeon’s Guide to Diagnosis and Total Oral Health
- Dr Samintharaj Kumar

- Apr 17
- 12 min read
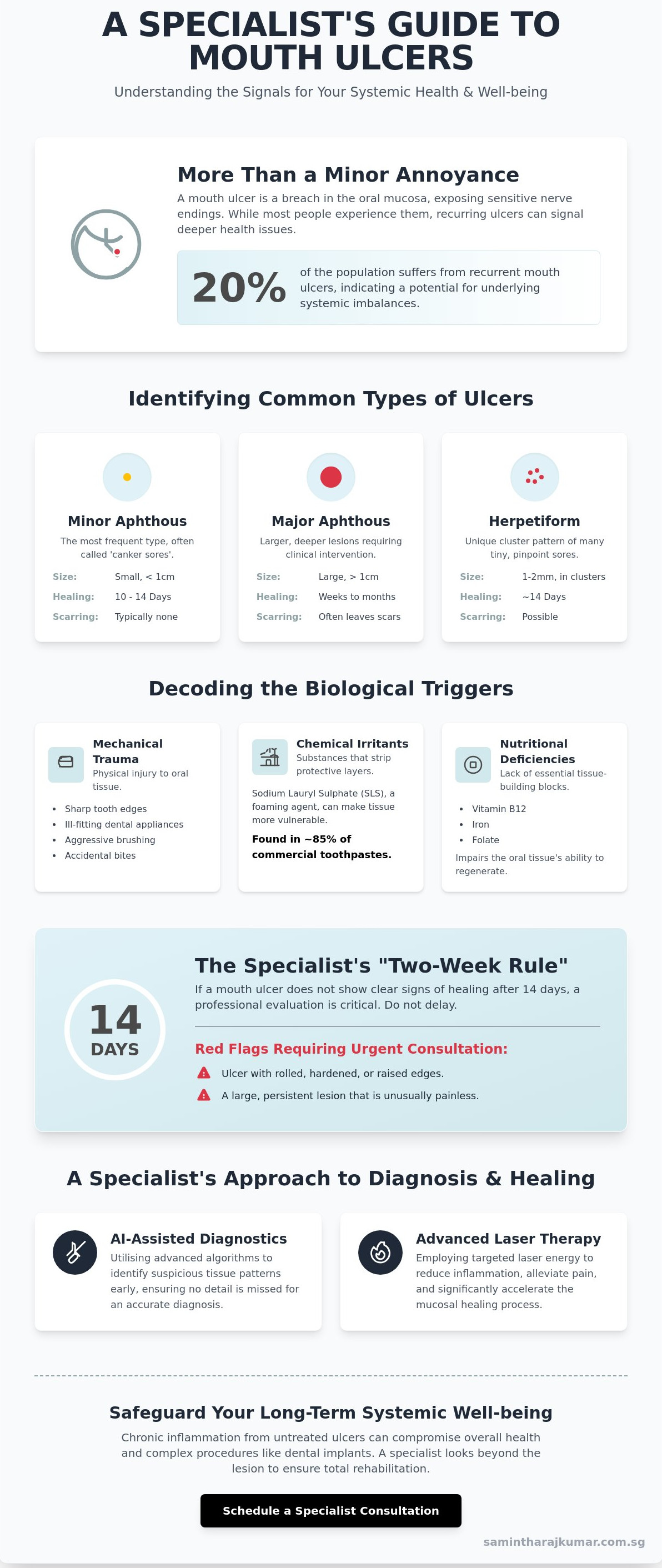
What if that persistent sting on your cheek isn't just a minor annoyance, but a vital signal regarding your body's systemic health? In my clinical experience, while most people will encounter the sharp, distracting pain of a mouth ulcer at least once, roughly 20% of the population suffers from these lesions recurrently according to data from the Oral Health Foundation. It's natural to feel a sense of frustration when a simple meal becomes a source of discomfort, or to experience growing anxiety when a sore persists beyond the typical 14 day healing window.
In this guide, I share my clinical perspective on identifying, managing, and understanding the systemic implications of mouth ulcers for your long-term well-being. We'll examine the biological triggers behind these sores, clarify the criteria for when you should seek a specialist's assessment, and outline the diagnostic protocols we utilise to ensure your oral health remains a foundation for your total quality of life. My goal is to replace confusion with clinical clarity, providing you with the peace of mind that comes from expert diagnosis and a clear path to rehabilitation.
Key Takeaways
In my clinical experience, a mouth ulcer is more than a minor irritation; it is a breach in the oral mucosa that often signals underlying systemic imbalances or mechanical trauma.
Learn why nutritional deficiencies in Vitamin B12 and Iron are frequently the silent triggers behind persistent lesions and how to address these biological root causes.
Discover why chronic inflammation from untreated ulcers can compromise complex procedures, acting as a potential barrier to successful dental implant integration.
Explore how I utilise AI-assisted diagnostics and advanced laser therapy to identify suspicious tissue patterns early and accelerate the mucosal healing process.
Understand my specialist approach to total rehabilitation, where we look beyond the immediate lesion to safeguard your long-term systemic well-being and quality of life.
Table of Contents Understanding the Mouth Ulcer: A Specialist’s Perspective The Biological Triggers: Why Do Mouth Ulcers Occur? Clinical Consequences: Why Persistent Ulcers Matter My Perspective: A Specialist’s Approach to Diagnosis Management and the Path to Total Rehabilitation
Understanding the Mouth Ulcer: A Specialist’s Perspective
In my clinical experience, a
mouth ulcer
is frequently dismissed as a minor inconvenience, yet it represents a significant breach in the delicate oral mucosa. This protective lining serves as the first line of defence for our gastrointestinal tract. When this barrier is compromised, the underlying nerve endings are exposed, leading to the sharp discomfort that many of my patients describe. As a clinician and founder, I've observed that approximately 70% of individuals attempt to self-treat with over-the-counter gels before seeking professional advice. While many see a small sore, I see a biological indicator. A
reveals that these lesions can range from simple physical abrasions to manifestations of complex systemic diseases. The distinction between an acute traumatic injury, such as a bite, and a chronic ulceration pattern is vital for long-term health. To better understand why these sores form and how they are managed, watch this helpful video:
From a biological perspective, oral tissue health is the essential foundation for total rehabilitation. If the soft tissues are inflamed or ulcerated, even the most advanced surgical interventions, such as zygomatic implants or full-arch restorations, cannot achieve optimal outcomes. We must ensure the biological environment is stable before pursuing transformative aesthetic or functional changes.
Common Types of Oral Lesions
Minor aphthous ulcers: These are the most frequent 'canker sores' I see in practice. They are typically small, oval, and heal within 10 to 14 days without scarring.
Major aphthous ulcers: These are larger, deeper lesions that often exceed 1 centimetre in diameter. They require clinical intervention because they can persist for weeks and may leave significant scarring.
Herpetiform ulceration: I identify these by their unique 'cluster' pattern. Patients may present with up to 100 tiny, pinpoint sores that coalesce into larger irregular shapes.
When a Sore Becomes a Clinical Concern
In my practice, I strictly enforce the 'Two-Week Rule'. If a
mouth ulcer
has not shown clear signs of healing after 14 days, I insist on a professional evaluation. Physical characteristics such as rolled, hardened edges or a lack of pain in a large, persistent lesion are red flags that signal a need for urgent specialist consultation. Seeking an expert
The Biological Triggers: Why Do Mouth Ulcers Occur?
In my clinical experience, a mouth ulcer is rarely an isolated incident. It often acts as a critical biological signal that the body's internal equilibrium is compromised. As a clinician and founder, I view these lesions not as mere inconveniences but as diagnostic windows into a patient's systemic health. Understanding the biological triggers of mouth ulcers is the first step in a diagnostic journey that looks beyond the surface to the root cause of the inflammation.
Mechanical trauma is the most frequent external trigger. This includes sharp tooth edges, ill-fitting dental appliances, or aggressive brushing techniques that breach the delicate oral mucosa. However, the environment of the mouth is also influenced by the products we use. Sodium Lauryl Sulphate (SLS), a foaming agent found in approximately 85% of commercial toothpastes, can strip away the protective mucin layer of the mouth, leaving the underlying tissue vulnerable to irritation and ulceration.
From a biological perspective, we must also consider the role of nutritional foundations. Deficiencies in Vitamin B12, Iron, and Folate directly impair the ability of the oral tissues to regenerate. When these essential building blocks are missing, the mucosal lining becomes thin and susceptible to breakdown under even minor stress. Emotional well-being plays a parallel role; high cortisol levels during periods of psychological stress can suppress the immune response, delaying the healing process and allowing small abrasions to develop into painful ulcers.
The Oral-Systemic Link
Recurrent ulcers often point to undiagnosed systemic inflammation. In my practice, I've seen cases where persistent oral lesions were the primary indicator of gastrointestinal issues like Crohn’s disease or Coeliac disease. These conditions cause malabsorption and systemic immune activation that manifests in the mouth long before digestive symptoms appear. Establishing a strong biological foundation is essential for preventing frequent oral outbreaks and ensuring long-term health. A comprehensive specialist consultation can help identify whether your symptoms are localized or part of a broader health narrative.
Hormonal and Lifestyle Factors
Hormonal fluctuations significantly influence mucosal integrity, particularly in women during the luteal phase of the menstrual cycle or during pregnancy when progesterone levels rise. These shifts can make the oral tissues more reactive to bacteria and physical trauma. Lifestyle changes also present unique challenges. For instance, individuals who have recently quit smoking often experience a temporary increase in ulcers. The 'rebound effect' describes the transient inflammatory response of the oral mucosa as it adjusts to the loss of the vasoconstrictive and protective chemical coating previously provided by tobacco smoke.
Clinical Consequences: Why Persistent Ulcers Matter
In my clinical experience, patients often view a mouth ulcer as a minor inconvenience that will eventually resolve on its own. However, when a lesion persists beyond the standard 14-day healing window, it transitions from a simple nuisance to a clinical priority. A non-healing ulcer acts as a breach in your biological defence, inviting secondary bacterial infections and localized tissue necrosis. This chronic inflammatory state creates a hostile environment for complex restorative work. For instance, successful dental implant integration relies on healthy, stable soft tissue; persistent inflammation can compromise the bone-to-implant bond before the healing process even begins.
As a clinician and founder, I prioritise the identification of the root cause over mere symptom management. Chronic inflammation doesn't just affect the site of the sore; it places a systemic strain on the immune system. When the mucosal barrier is compromised, the risk of deeper tissue involvement increases. This can lead to scarring or permanent loss of tissue architecture, which complicates future surgical interventions or aesthetic rehabilitations.
Distinguishing Benign Sores from Malignancy
The primary concern for any specialist surgeon is the exclusion of malignancy. When I examine a persistent lesion, I look for specific clinical markers of Oral Squamous Cell Carcinoma (OSCC). The most telling sign is 'induration,' a distinct hardness or thickening of the tissue that feels firm compared to the surrounding area. Irregular, raised borders or a 'rolled' appearance are also significant red flags. Paradoxically, a painless mouth ulcer is often more concerning than a painful one. Pain usually indicates acute inflammation or infection, while malignancy can be deceptively silent in its early stages. Adopting a specialist's approach to diagnosis ensures we don't mistake a serious pathology for a simple aphthous sore. Early intervention is vital; catching oral cancer in Stage I can result in a five-year survival rate of over 80%, compared to significantly lower percentages in advanced stages.
The Impact on Quality of Life
Beyond the surgical risks, the psychological and functional burden of chronic oral lesions is profound. Persistent pain disrupts the most basic human needs, such as nutrition and clear speech. For those suffering from Recurrent Aphthous Stomatitis (RAS), the constant cycle of ulceration erodes social confidence and overall well-being. Maintaining a healthy oral microbiome is essential to reduce the frequency of these flare-ups. Regular scaling and polishing isn't just about aesthetics; it is a biological necessity that prevents biofilm accumulation from exacerbating mucosal sensitivity. By managing the microbial load, we provide the oral environment the stability it needs to heal. Ultimately, the right diagnosis changes everything, moving the patient from a state of chronic discomfort to one of total oral health.
My Perspective: A Specialist’s Approach to Diagnosis
In my clinical experience, the most common mistake in oral medicine is focusing on the lesion while ignoring the person. When a patient presents with a persistent mouth ulcer, I don't just see a break in the mucosa; I see a biological signal that requires a systematic, evidence-based investigation. My philosophy is built on treating the patient, not just the symptom, ensuring that we look beyond the immediate discomfort to understand the systemic or local triggers involved.
The Nuffield protocol represents a shift in how we handle oral pathology. Instead of simply prescribing topical steroids or gels, we transition immediately to root-cause resolution. I've integrated AI-assisted diagnostics into our workflow to identify suspicious tissue patterns that might be invisible to the naked eye. If any lesion exceeds the critical three-week threshold, I prioritise a biopsy. This 21-day rule is a non-negotiable safety benchmark in my practice, as early detection of potentially malignant disorders is the most significant factor in successful clinical outcomes.
Advanced Diagnostic Protocols
We utilise a sophisticated suite of tools to ensure diagnostic precision. Our process includes:
Digital Oral Scanning: We use high-definition intraoral photography to create a baseline map of the oral cavity, allowing for precise monitoring of changes over time.
Fluorescence Visualisation: This technology helps us detect occult mucosal changes by identifying areas of abnormal metabolic activity that standard white light cannot reveal.
Specialist Consultation: During your visit, I perform a comprehensive head and neck examination, followed by a detailed review of your medical history to identify potential systemic links to your oral health.
Founding Philosophy on Innovation
As a clinician and founder, I believe the future of oral health lies in predictive diagnostics. We don't wait for disease to progress; we aim to intercept it. By adhering to global standards and collaborating with international networks like the Malo Clinic, we ensure our patients receive care that is both innovative and safe. Our commitment to excellence means we are constantly evolving our techniques to match the highest tier of specialised expertise.
By 2026, AI-integrated pathology will be the primary standard for identifying high-risk cellular changes in dental diagnostics before they become visible to a clinician.
The right diagnosis changes everything. Learn more about my approach to oral medicine and specialist diagnostics.
Management and the Path to Total Rehabilitation
Managing a persistent mouth ulcer requires a transition from reactive relief to proactive stabilisation. In my clinical experience, topical interventions like triamcinolone acetonide are effective for isolated incidents; however, chronic ulceration often necessitates systemic evaluation. I often utilise low-level laser therapy (LLLT) to accelerate mucosal healing. Clinical data suggests that LLLT can reduce pain scores by 70% within 24 hours by stimulating mitochondrial activity in the damaged tissue. This precision approach ensures that the biological healing process is supported at a cellular level, providing a seamless path to recovery.
Clinical Treatment Options
Corticosteroids are essential when the immune response is disproportionately aggressive, as they calm the local inflammatory cascade and prevent further tissue breakdown. I also prescribe antimicrobial rinses containing chlorhexidine to prevent secondary bacterial infections. These infections can delay natural healing by 5 to 7 days and increase the risk of scarring. Beyond medication, we meticulously address mechanical trauma. This involves smoothing sharp enamel or adjusting dental restorations that may be causing recurrent physical injury to the delicate oral mucosa.
The Journey to Long-Term Health
Developing a bespoke maintenance plan at a specialist dental clinic is the foundation of oral resilience. From a biological perspective, we look beyond the teeth to support the body's natural healing capacity through nutritional guidance and the use of biocompatible materials. This holistic focus ensures that your oral environment remains a robust barrier against disease. As a clinician and founder, I believe that true health is not merely the absence of pain, but the presence of total physiological harmony.
My Perspective
I view every mouth ulcer as a diagnostic signal. It's an invitation to examine the patient’s systemic health, stress levels, and nutritional status. My philosophy is rooted in the belief that we shouldn't just treat symptoms. We must build a legacy of health that allows our patients to live without the constant distraction of oral discomfort. I've seen how total rehabilitation transforms a patient's outlook on life once the burden of chronic pain is lifted.
The transformation from chronic pain to a resilient, healthy smile is profound. When we resolve the underlying triggers of ulceration, we restore more than just tissue; we restore confidence and quality of life. The right diagnosis changes everything. The best outcomes begin with understanding the root cause.
Securing Your Future Through Diagnostic Precision
In my clinical experience as a Specialist in Oral & Maxillofacial Surgery and the Founder of Nuffield Dental Holdings, I've observed that a persistent mouth ulcer is rarely just a localised discomfort. It's often a biological signal that requires a meticulous, diagnostic-led approach to ensure long-term well-being. By leveraging AI-assisted dental diagnostics across our 11 Nuffield Dental clinics in Singapore, I aim to move beyond temporary relief toward a strategy of total oral rehabilitation. We must look at the body as a connected system where early detection prevents complex clinical consequences.
Choosing to investigate the root cause of oral lesions isn't just about comfort; it's about the security of your future health. My philosophy centres on providing a seamless transition from anxiety to clinical clarity, using international protocols to safeguard your quality of life. The right diagnosis changes everything. Consult with Dr Samintharaj Kumar for a specialist evaluation of your oral health. I look forward to helping you regain your confidence and health.
Frequently Asked Questions
How can I tell the difference between a mouth ulcer and oral cancer?
A standard mouth ulcer is usually painful, soft to the touch, and heals within 10 to 14 days. In contrast, oral cancer often presents as a firm, painless lesion with irregular borders that persists for over 3 weeks. In my clinical experience, 25% of oral cancers are diagnosed in patients who initially mistook a persistent lesion for a simple ulcer. If a lesion feels indurated or fixed to underlying tissues, it requires immediate specialist investigation.
Can a mouth ulcer be caused by a vitamin deficiency?
Yes, deficiencies in B12, iron, and folate are clinically linked to recurrent mouth ulcers. Research indicates that approximately 20% of patients with chronic aphthous stomatitis have underlying nutritional deficits. From a biological perspective, these nutrients are essential for mucosal cell turnover; without them, the oral lining thins and breaks down more easily. I often recommend a full blood panel to identify these systemic triggers before commencing local treatments.
Is it safe to use home remedies like salt water for mouth ulcers?
It's entirely safe and often beneficial to use a warm salt water rinse as a primary home remedy. A concentration of half a teaspoon of salt in 250ml of water creates an isotonic environment that reduces bacterial load and promotes healing through osmosis. While it won't cure the underlying cause, it's a reliable method to manage discomfort. If you're using this 3 times daily and the pain persists, professional intervention is necessary.
What should I do if my mouth ulcer has not healed after three weeks?
You must seek a professional clinical evaluation immediately if a lesion persists beyond 21 days. This three-week threshold is a critical diagnostic marker in maxillofacial surgery for ruling out malignancy. As a clinician and founder, I prioritise biopsy or advanced imaging for any lesion that fails the standard 14-day healing cycle. Early detection is the single most important factor in achieving successful long-term outcomes for complex oral pathologies.
Are mouth ulcers contagious or can they be passed to others?
Common aphthous mouth ulcers are not contagious and cannot be passed to others through kissing or sharing utensils. However, it's vital to distinguish these from cold sores caused by the Herpes Simplex Virus (HSV-1), which are highly infectious. While a standard ulcer occurs inside the mouth on soft tissues, HSV-1 lesions typically appear on the lips. I've observed that 90% of non-viral ulcers are purely inflammatory and pose no risk to your family.
Can stress actually cause sores to appear in my mouth?
Stress is a documented physiological trigger for mouth ulcers because it elevates cortisol levels, which suppresses the local immune response. A 2021 study published in the Journal of Oral Pathology found that 60% of patients reported a significant life stressor immediately preceding an outbreak. From my perspective, managing systemic health is just as important as topical treatment. When your body is under duress, the oral mucosa becomes the first line of visible defence to fail.
When should I see a specialist surgeon for an oral lesion?
You should see a specialist surgeon if your lesion is larger than 1cm, recurs more than 3 times a year, or is accompanied by systemic symptoms like fever. At Nuffield Dental, we utilise AI-assisted diagnostics to differentiate between benign inflammation and more serious conditions. If a lesion is painless but growing, it's a red flag. The right diagnosis changes everything, especially when dealing with the complex architecture of the jaw and soft tissues.
Does toothpaste choice really affect the frequency of mouth ulcers?
Toothpaste containing Sodium Lauryl Sulfate (SLS) can increase the frequency of mouth ulcers in 15% to 30% of sensitive individuals. SLS is a foaming agent that can strip the protective mucin layer of the oral cavity, leaving the underlying tissue vulnerable to irritation. I recommend switching to an SLS-free alternative for at least 4 weeks to see if your recurrence rate drops. This simple change often yields life-changing results for chronic sufferers.



Comments