
Nerve Repositioning for Dental Implants: A Surgeon’s Perspective on Advanced Mandibular Rehabilitation
- Dr Samintharaj Kumar

- 2 days ago
- 12 min read
What if the very nerve that seems to block your path to a permanent smile could be precisely moved to make room for your restoration? In my clinical experience, many patients arrive at my practice feeling defeated after being told their lower jaw bone is too thin or too close to the alveolar nerve for traditional surgery. It's a distressing position to be in, especially when you're seeking a long-term solution for missing teeth. However, nerve repositioning for dental implants is a sophisticated biological intervention that allows us to create space where nature has retreated, offering hope to those with extreme bone resorption.
I understand that the thought of moving a major facial nerve can be daunting, and the fear of permanent numbness is a valid concern that I take very seriously. This guide serves as an expert-led deep dive into the surgical mastery required for advanced mandibular rehabilitation. I'll explain the vital differences between nerve lateralisation and transposition, while outlining the rigorous protocols I use to prioritise your safety. By the end, you'll have the clarity needed to understand if you're a candidate for this transformative procedure and the confidence that comes from knowing exactly how we protect your long-term functional excellence.
Key Takeaways
Learn why severe bone loss in the lower jaw doesn't mean you're ineligible for a permanent smile, provided the right surgical expertise is applied.
Understand how nerve repositioning for dental implants works as a sophisticated biological intervention to safely bypass anatomical limitations.
Discover why I prioritise AI-assisted 3D imaging and CBCT scans to map your unique anatomy with millimetre precision before any procedure begins.
Grasp the clinical differences between nerve lateralisation and transposition, and how these choices impact your long-term functional outcome.
Gain clarity on the recovery process, including how we manage neurosensory changes like paresthesia to prioritise your long-term well-being.
Table of Contents
Understanding the Challenge: When Bone Atrophy Meets Nerve Proximity
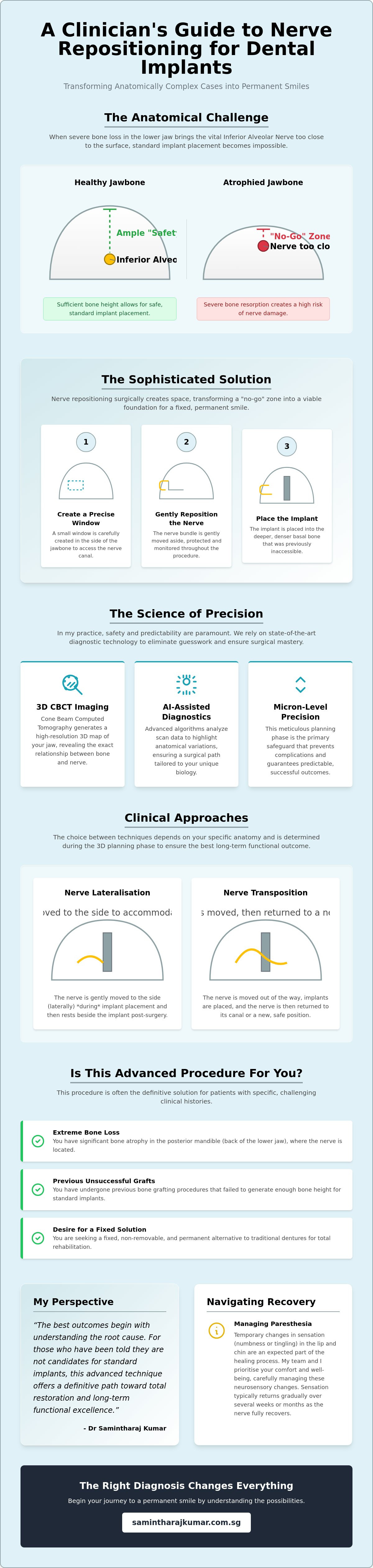
In my clinical experience, the most significant hurdle in lower jaw reconstruction isn't just the lack of bone. It's the location of the Inferior Alveolar Nerve (IAN). This vital structure runs through the mandible, providing sensation to your lower lip, chin, and teeth. When years of tooth loss cause the alveolar ridge to resorb, the bone essentially melts away, leaving the nerve mere millimetres from the surface. Standard implantology requires a "safety zone" of bone height to avoid nerve impingement. Without this clearance, placing a traditional implant is impossible without risking permanent sensory damage.
To overcome this anatomical barrier, I utilise a technique known as nerve repositioning for dental implants. This surgical procedure involves creating a precise window in the side of the jawbone to gently move the nerve bundle aside. By doing so, I can place the implant into the deeper, denser bone of the jaw base that was previously inaccessible. It's a meticulous process that transforms a "no-go" zone into a viable foundation for a fixed smile, effectively bypassing the limitations of natural bone loss.
To better understand how this procedure looks from a surgical and patient standpoint, watch this helpful video:
The Role of the Inferior Alveolar Nerve
From a biological perspective, the IAN is the sensory lifeline for the lower face. Its proximity to the crest of the jaw prevents standard dental implant placement because the titanium post would need to occupy the same space as the nerve. If we leave bone atrophy untreated, the jaw continues to thin, which can eventually lead to discomfort even when wearing simple dentures. The biological consequence of ignoring this atrophy is a progressive loss of facial structure and functional bite strength.
Identifying Candidates for Nerve Repositioning
I typically identify candidates for nerve repositioning for dental implants based on the severity of their mandibular atrophy. This procedure is often the definitive solution for patients who have:
Extreme bone loss in the posterior mandible (the back of the lower jaw).
Undergone previous bone grafting procedures that failed to provide enough height.
A strong desire for a fixed, non-removable alternative to traditional dentures.
My philosophy is that the best outcomes begin with understanding the root cause of bone loss. For those who have been told they aren't candidates for standard implants, this advanced technique offers a path toward total restoration.
The Science of Precision: Mapping the Nerve with AI and 3D Imaging
From a biological perspective, relying on traditional 2D X-rays for nerve repositioning for dental implants is simply not an option. A flat image cannot convey the complex, three-dimensional relationship between the nerve canal and the surrounding cortical bone. Instead, I utilise Cone Beam Computed Tomography (CBCT) to generate a high-resolution 3D map of the jaw. This allows me to measure the exact volume of available bone and the precise depth of the nerve bundle before I even pick up a surgical instrument. It's a level of detail that transforms a complex surgery into a predictable procedure.
Modern AI-assisted diagnostics have further refined this process. By applying advanced algorithms to CBCT data, we can visualise anatomical variations that might be missed by the human eye alone. This level of detail is essential when applying a new clinical classification system to determine the safest surgical path for each individual. Micron-level precision in the planning phase is the primary safeguard that prevents intra-operative complications and ensures predictable results. In my clinical experience, this digital foresight is what allows us to treat patients who were previously told their cases were too high-risk.
Biological Preservation Protocols
Protecting the neurovascular bundle requires more than just a steady hand; it requires specialised technology. In my practice, I use piezoelectric surgery, which employs ultrasonic vibrations to cut through hard mineralised bone while leaving soft tissues, such as nerve fibres, completely unharmed. These tools are designed to distinguish between different tissue densities, providing an extra layer of biological safety during the delicate surgical access phase. It's about minimising trauma to ensure a smoother, faster healing response for the patient.
Digital Surgical Guides
Once the mapping is complete, I create a digital surgical guide that acts as a physical roadmap during the procedure. This guide ensures that every drill movement and implant placement avoids the nerve path with absolute certainty. I've found that this digital synergy is particularly effective when working with biocompatible materials like ceramic dental implants, which support a healthy gingival response and long-term stability. Digital planning doesn't just improve accuracy; it significantly reduces surgery time, which is a key factor in reducing post-operative swelling and discomfort. The best outcomes begin with understanding the root cause, and you can learn more about our philosophy on comprehensive restoration by exploring our clinical protocols.
Nerve Repositioning vs. Lateralisation: A Clinical Comparison
As a clinician, I categorise these techniques based on how we handle the nerve bundle and where the implant eventually sits. While both fall under the umbrella of advanced mandibular rehabilitation, they are distinct surgical pathways. In nerve lateralisation, I create a small window in the bone and gently move the nerve to the side. This allows me to place the implant "past" the original canal, anchoring it into the dense basal bone. It's a precise manoeuvre that preserves the nerve's integrity while creating a stable foundation for your new teeth.
Conversely, nerve repositioning, often referred to as transposition, is a more involved procedure that typically involves the mental foramen, the exit point of the nerve. Here, the nerve is moved so the implant can be placed "through" the space where the canal once was. Determining which approach is safer depends entirely on your specific anatomy. Lateralisation is often my preference for the posterior mandible because it involves a smaller surgical window. However, nerve repositioning for dental implants becomes essential if the bone loss extends toward the front of the mouth. In either case, the goal is to achieve primary stability without compromising long-term sensory health.
Comparing the Techniques
The decision-making process is never arbitrary. In my clinical experience, lateralisation tends to carry a slightly lower risk of permanent sensory changes because we aren't manipulating the nerve's exit point. Repositioning is a more extensive procedure. It offers greater flexibility for implant placement but requires a higher level of surgical mastery to manage the neurovascular bundle. I choose the technique that provides the most robust foundation for your restoration while minimising biological stress. Every millimetre of movement is planned in advance using the 3D mapping I discussed earlier.
Alternatives to Nerve Manipulation
We don't always need to move the nerve to achieve a successful outcome. From a biological perspective, I always explore more conservative routes first. Short implants, often 6mm or less, can sometimes bypass the need for nerve repositioning for dental implants entirely if there is enough residual height. For patients requiring total oral restoration, we might incorporate zygomatic dental implants to provide stability in the upper jaw while using alternative techniques in the lower. Additionally, vertical ridge augmentation, which involves building the bone upwards rather than moving the nerve, remains a viable alternative. The right choice depends on your timeline, bone quality, and desired functional outcome. The best outcomes begin with understanding the root cause of bone loss.
Navigating Recovery: Paresthesia, Healing, and Patient Expectations
Healing is a biological journey that requires patience and strict adherence to clinical protocols. In my clinical experience, the primary concern patients voice regarding nerve repositioning for dental implants is the risk of paresthesia. It is a valid fear, but it's one that we manage through meticulous planning and post-operative care. Paresthesia refers to an altered sensation, such as numbness or tingling, in the lower lip and chin. While this can be startling, it is important to distinguish between a temporary physiological response and permanent nerve damage.
Temporary numbness is often a sign of the nerve "sleeping" after manipulation rather than being damaged. During the surgery, the neurovascular bundle is gently moved, which can lead to a period of reduced conductivity. From a biological perspective, the first 48 hours are dedicated to managing the initial inflammatory response, whereas the actual nerve regeneration occurs over a much longer horizon. Data from a systematic review indicates that 99.47% of patients experience only temporary neurosensory disturbances, with the vast majority recovering fully within six months. Only a very small fraction, approximately 0.53%, report permanent changes, which highlights why specialist mastery is so critical for this procedure.
The Clinical Checklist for Post-Op Care
Managing swelling and discomfort requires a proactive approach. I provide my patients with specialist-prescribed protocols that include specific anti-inflammatory medications and cold therapy. You can follow my detailed checklist for managing swelling after tooth extraction to guide your immediate care. Dietary restrictions are equally vital during this time. Soft foods are non-negotiable during the initial integration phase because they prevent mechanical stress on the healing bone and the newly repositioned nerve bundle.
Monitoring Nerve Regeneration
I often incorporate Vitamin B complexes and specific neurotrophic factors into the recovery plan to support nerve health and accelerate the healing of the protective sheath. We schedule regular follow-up intervals to monitor your sensory response through clinical testing, ensuring that your recovery is progressing as expected. Patients often ask when they can safely resume exercise after oral surgery; while light walking is encouraged early on, strenuous activity must be avoided until I have confirmed the stability of the surgical site. The best outcomes begin with understanding the root cause of your concerns, and I encourage you to reach out to my team for a personalised assessment of your suitability for this advanced rehabilitation.
My Perspective: Total Rehabilitation and the Future of Care
As a clinician and founder, I believe that the best outcomes begin with understanding the root cause of bone loss. In my clinical experience, many patients focus solely on the gap in their smile, but the underlying issue is often the progressive collapse of the jaw's structural foundation. We don't just place implants. My philosophy is rooted in the belief that we must restore the architectural integrity of the face. Nerve repositioning for dental implants is a prime example of how we push the boundaries of modern medicine to ensure a patient doesn't have to settle for compromised, removable solutions.
From a biological perspective, the intersection of AI-assisted diagnostics, biological dentistry, and surgical mastery represents the future of our field. By using technology to map the jaw with absolute precision, I can execute complex procedures that were once considered too high-risk for the average practice. I prioritise long-term quality of life over quick fixes because your health is a legacy, not a transaction. This meticulous approach is the cornerstone of Nuffield Dental, where we've built an institution of excellence dedicated to solving the most complex oral rehabilitation cases in the region.
The Psychological Impact of Restored Function
The journey from the persistent anxiety of "failing teeth" to the quiet confidence of a stable bite is profound. When we restore the lower jaw through nerve repositioning for dental implants, we aren't just giving you back the ability to chew; we're restoring facial aesthetics and youthful volume that bone loss often takes away. A well-supported jaw maintains the natural contours of the face, preventing the prematurely aged appearance associated with extreme resorption. It's about more than function. It's about the emotional renewal that comes with feeling whole again and the confidence to engage with the world without hesitation.
Conclusion: Taking the Next Step
The importance of a comprehensive consultation with a specialist oral surgeon cannot be overstated. In complex cases where the bone has thinned significantly, the right diagnosis changes everything. It's the difference between being told "it's impossible" and being given a clear, evidence-based roadmap to a permanent solution. Final outcomes are always built on a foundation of trust and technical excellence. If you've been searching for a way forward, remember that your journey toward restoration starts with a single, expert-led conversation. The best outcomes begin with understanding the root cause, and I invite you to discover how our specialised protocols can transform your long-term well-being.
Restoring Your Confidence Through Clinical Mastery
Navigating the complexities of advanced bone loss requires more than just technical skill; it demands a visionary approach to biological restoration. We've explored how AI-assisted 3D mapping and specialised technology have transformed nerve repositioning for dental implants from a high-risk procedure into a predictable, life-changing intervention. By prioritising the architectural integrity of your face, we can move beyond the limitations of traditional dentistry to provide a fixed, stable smile where others see only obstacles.
As the founder of Nuffield Dental Holdings and a specialist in Zygomatic and All-on-4 protocols, I've dedicated my practice to refining AI-assisted surgical diagnostics for the most complex cases. My goal is to replace the anxiety of being rejected for standard implants with the security of expert-led care. Every successful rehabilitation is built on a foundation of precision and personal accountability. The best outcomes begin with understanding the root cause. Explore the future of oral rehabilitation with Dr Samintharaj Kumar and begin your journey toward a functional, vibrant legacy.
Frequently Asked Questions
Is nerve repositioning for dental implants a safe procedure?
Yes, it is a safe and highly predictable procedure when performed by a specialist oral surgeon using advanced 3D diagnostics. While it is more complex than standard implantology, the risk of permanent complications is exceptionally low. In my clinical experience, using AI-assisted planning allows us to navigate the jaw's anatomy with a level of precision that ensures the safety of the neurovascular bundle.
How much does nerve repositioning cost in Singapore?
The cost of this procedure varies based on the complexity of your specific case and the surgical techniques required to achieve a successful outcome. Factors such as the use of piezoelectric surgery or the need for supplemental bone grafting will influence the final investment. I recommend a comprehensive consultation to receive a personalised clinical roadmap and a detailed breakdown of the requirements for your rehabilitation.
What is the success rate of dental implants after nerve repositioning?
Dental implants placed following this procedure have a high success rate, with studies showing between 95% and 98% success. A meta-analysis from 2024 specifically found a 97% success rate at the ten year mark. From a biological perspective, these results are possible because the technique allows the implant to be anchored into the dense, high-quality basal bone of the mandible.
Can nerve repositioning cause permanent facial paralysis?
No, nerve repositioning for dental implants cannot cause facial paralysis because the Inferior Alveolar Nerve is a sensory nerve rather than a motor nerve. It provides sensation to the lower lip and chin but does not control the muscles used for facial expressions. While temporary sensory changes are possible, your ability to move your face and smile will remain completely unaffected.
How long does the numbness last after nerve repositioning surgery?
Most patients see a full return of sensation within three to six months as the nerve regenerates. Research indicates that 88.9% of patients recover from neurosensory disturbances by the six month mark. While the nerve may "sleep" initially after manipulation, a systematic review found that 99.47% of these disturbances are temporary and resolve during the standard healing journey.
Are there alternatives to nerve repositioning for lower jaw implants?
Yes, there are several alternatives that we explore based on your unique bone volume. We may consider using short implants that are 6mm or less in length or performing vertical bone grafting to increase the available height. In some cases of full mouth reconstruction, I might suggest using zygomatic dental implants in the upper jaw to simplify the overall treatment plan for the lower jaw.
What happens if the inferior alveolar nerve is damaged during surgery?
If the nerve experiences minor trauma or compression, it typically leads to a temporary period of altered sensation that resolves as the area heals. In my practice, I mitigate this risk by using ultrasonic bone-cutting tools that are designed to protect soft tissues and nerve fibres. If significant damage were to occur, specialised microsurgical techniques are available to repair the nerve and restore its function.
How do I know if I need nerve repositioning for my implants?
You may require nerve repositioning for dental implants if a 3D CBCT scan shows that your lower jaw bone has resorbed to a point where there is insufficient height above the nerve canal. If you have previously been told that you are not a candidate for implants due to nerve proximity, this advanced procedure is often the definitive solution. A specialist assessment is necessary to confirm your candidacy.



Comments